|
BOOK NOW |
ASK ABOUT YOUR PAIN |
Home > Blog > Physiotherapy > Conditions > Shoulder Pain > Shoulder Blade Pain > Shoulder Fracture Physiotherapy
Shoulder Fracture Physiotherapy
A shoulder fracture happens when one of the shoulder bones breaks into two or more pieces.
Shoulder fractures may occur at the
- clavicle (collar bone)
- proximal humerus fracture or midshaft humeral fracture (upper arm bone) or the
- scapula (shoulder blade)
Shoulder fractures may be categorized as
- non-displaced fracture, where it is typically considered a "stable fracture" and the broken bone remains in its usual position
- displaced fracture, where it has moved out of position by at least 1 cm.
If the bone has broken in to three or more pieces it is known as a comminuted shoulder fracture.
Thankfully, in most cases, a broken shoulder does not require surgery.
What is normally done for stable undisplaced shoulder fractures, the patient's affected arm will be supported in a sling initially to
- protect the fracture and fracture site
- to allow it to heal
- followed with a shoulder fracture physiotherapy rehab program under the guidance of our senior physical therapist.
Types Of Shoulder Fracture
The most common shoulder fracture in children is a fractured clavicle aka broken collar bone.
For us adults, the most common shoulder fracture is a proximal humerus fracture which is a break in the upper arm bone; and the least common shoulder bone to break is the scapula bone which is commonly known as the shoulder blade.
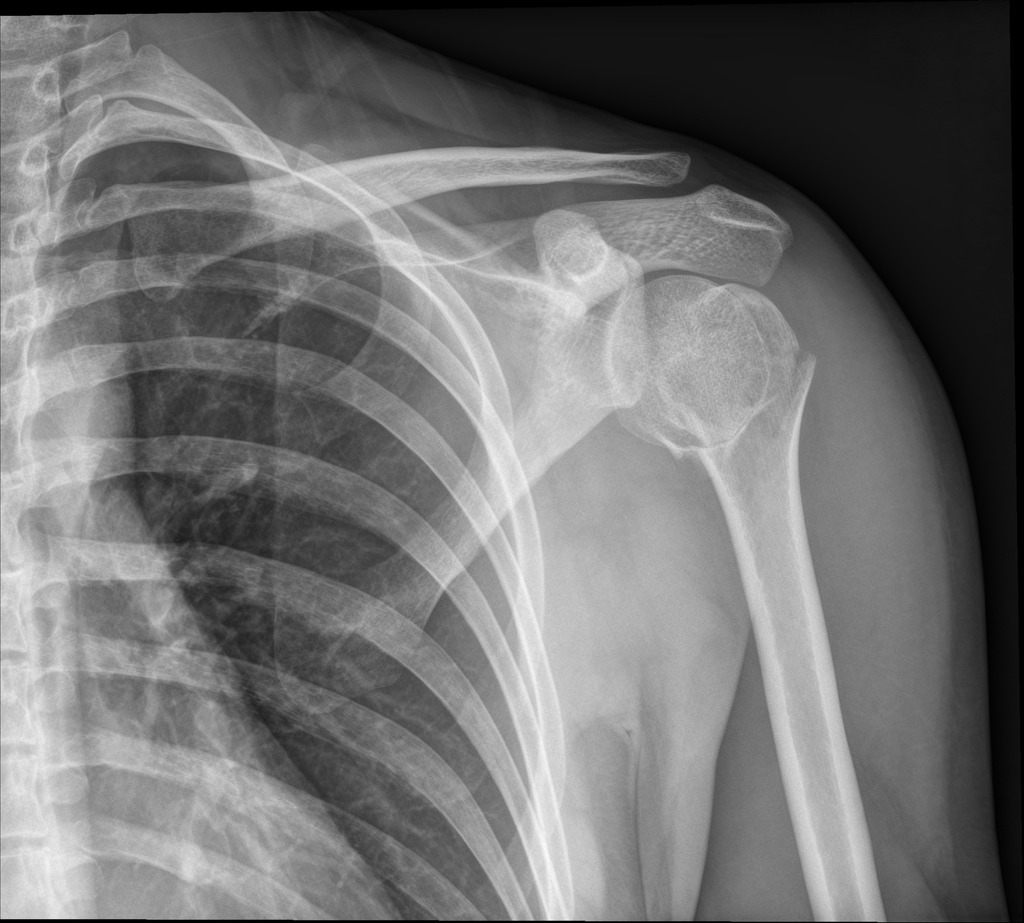
Clavicle Fractures
Our clavicle/collar bone is a thin, long-ish bone found at the front of the shoulder just in front of the top of the rib cage. It connects our sternum (which is our breastbone) to our scapula (the shoulder blade).
Clavicle fractures are not only the most common type of shoulder fracture in children, the collar bone is actually the most common bone in the whole body that kids break.
Thankfully again, clavicle fractures typically heal really well without the need for surgery, although they can be very painful for a couple of weeks, and during this time, can cause a lot of discomfort and inconvenience.
What Causes Clavicle Fractures?
Most of the time, collar bone fractures are caused by:
1) Falls
A simple fall either
- onto the side of the shoulder or
- falling onto the arm when the arm is outstretched
In fact, patients don’t have to fall very far to break their collarbones, it's moreso falling at a
- bad angle
- enough force
- which surface you land on
Even falling onto the side by accident can cause it!

2) Contact:
A sudden, strong direct blow to the collar bone can break it such as
- motor vehicle accidents
- sports injuries such as rugby or soccer
3) Birth:
Once in a while, babies can get shoulder fractures (especially clavicular fractures), during childbirth. What happens is that when babies are born in breech position (our 1st kid, Olivia was a breech baby too!) where the babies bottom comes out first instead of their head.
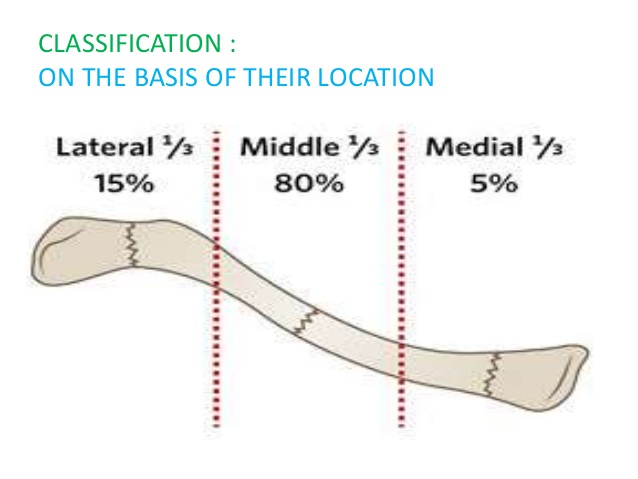
For collar bone or clavicle fractures, there are three general groups/types: depending on which part of the bone is broken. The most common is a type 1 fracture, where the break is located in the middle third of the bone, as this is the weakest part of the bone.
Humerus Fractures

Our humerus is the long bone in the upper arm that is located between our elbow and our shoulder. The very top of the humerus forms a ball shape known as the humeral head that rests in a socket formed by the shoulder blade.
Humerus fractures fall into three categories:
- Proximal Humerus Fractures:
The most common place to break the humerus is right smack at the top at the humeral head.
In fact, it is these types of proximal humerus fractures that account for approximately 5% of all fractures reported and are the most common type of shoulder fracture in patients who are above 65 years of age. - Humeral Shaft Fracture:
Refers to the breakage of the humeral bone anywhere in the middle section of the long humerus bone.
Often there may be associated damage to the surrounding nerves or blood vessels. Humeral shaft fractures is also very common, accounting for 3% of all fractures - Distal Humerus Fracture:
Refers to a break towards the bottom of the humerus bone, nearer to the elbow
Causes Of Humeral Fractures
Most of the time...humerus fractures happen by falls and falling over.
You see, our body's natural protective mechanism ensures that whenever we fall, we reflexively and automatically extend our hands to "break our fall" to prevent injury to our head (yeah it's something like a "sacrificing something to protect the more important stuff"), but falling onto an outstretched arm typically leads to humeral fractures.
A direct blow to the humerus or torsion-type force (rotational force) through it can also cause the bone to break, if the force is strong enough.
Most of the time, humeral fractures
- affect patients above 65 years of age
- 2x more common in women compared to men (2:1 ratio)
What happens is that with age and time, our bone density becomes lesser, meaning that our bones becomes more weak and brittle, and less force is required to have bone fractures. If there is any low bone density issues, or worse, osteoporosis - it makes the bones much easier to fracture.
To make matters worse, as we age, our muscles shrink a little and our balance becomes worse and vision/eyesight too, and in some cases, increased risks of dizziness - all adding to increased falls and fracture risks.
Compared to younger people, their bones are healthier and stronger so it'd require a high energy trauma for the humerus to break, such as
- falling from a tree
- motor vehicle accidents
- sports injuries
and that's why when it involves the younger population, their injuries tend to be more serious.
Shoulder Blade Fractures
Also known as scapular fractures, shoulder blade fractures are really rare amongst all the shoulder fractures.
The reason for this is because the bone is:
- located at the back part of the body, top of the rib cage, making it kind of hard to access or hit
- it is quite strong and well protected so it will take a lot of force to cause it to fracture
Most of the time, our shoulder blades are very rarely damaged by itself in isolation; they tend to be coupled with other hand, chest or back injury which can be very serious such as
- lung damage
- broken ribs
- shoulder complex
- spine fracture
- etc
Scapula fractures are rare and account for less than 1% of all fractures.
Although any parts of our shoulder blade can be broken or fractured, but most of the time, it is the body of the scapula that is injured rather than the neck or spine (the body of the scapular is weaker compared to the other 2).
Causes Of Scapular Fractures
Shoulder blade fractures are typically caused by
- motor-vehicle accidents such as motorbike collisions or high speed accidents
- sports injuries
- work injuries
- falls from height
Rare
The shoulder blade can also break during a seizure or from an electric shock as these can cause the muscles that control the shoulder blade to contract powerfully in different directions, pulling on the bone.
Shoulder blade fractures most commonly happen to patients who are between the ages of 25 and 40.
Symptoms Of Shoulder Fractures
If you have a shoulder fracture, you will likely already be aware of it and highly likely you can pinpoint or recall what exactly caused the injury. Regardless, whichever bone you have broken, patients will always experience a sharp pain at the time of injury which gives way to an ongoing dull ache.
The pain from shoulder fractures typically worsens with forms of arm movement, especially with shoulder involvement eg
- when trying to lift your arm above your head
- when any pressure is placed on the affected area
- or even when taking a deep breath (a full deep breath may cause the rib cage to expand and push at the fractured site of the shoulder blade)
Arm movement will almost certainly be restricted with presence of extensive bruising.
Specific symptoms for the different types of shoulder fracture include:
- Clavicle Fractures: A bulge over the broken area and a snapping or grinding noise when you move your arm
- Humerus Fractures: Severe swelling and bruising in the upper arm and there may be an obvious deformity
- Scapula Fractures: Bruising over the shoulder blade region. In approximately 80% of cases of scapula fractures there are associated injuries to the shoulder, spine, head, rib cage and/or lungs which may be very serious.
Treatment For Shoulder Fractures
Typically, if the shoulder fracture is stable and has zero or very minimal displacement, then most likely do not require corrective shoulder surgery. In that case, patients will require conservative management which will include:

1) Sling
Patients should have their affected shoulder protected and immobilized in a shoulder sling for at least 14 days (usually extended to up to 4-6 weeks), to
- protect the shoulder
- give a signal to others to avoid the injured site/arm
- decrease/prevent any additional force
Depending on which bone is broken, the type of sling will differ:
After a shoulder fracture the arm will be immobilised in a sling for at least the first 10-14 days and often 3-4 weeks, sometimes more, to allow the fracture to heal.
The type of sling will depend on which bone has been broken
- Clavicle Fracture
A figure of 8 sling is a popular choice with clavicle fractures as it immobilises the collar bone while supporting the shoulders and upper back to ensure good posture - Humeral Fracture:
Proximal humerus fractures are treated initially with an immboliser sling to support the fracture as it heals. Humeral shaft fractures are usually treated with a brace and a collar and cuff style sling rather than a triangular sling.
This is because by leaving the elbow unsupported, gravity and the weight of the arm draws the humerus downwards helping the bone to heal in the correct position.
If there is pressure up through the elbow, it can displace the bone causing it to heal in the wrong position. - Scapula Fracture:
A sling and shoulder immobiliser is typically used with shoulder blade fractures to keep the arm supported and close to the body.

2) Medication
If you have consulted a doctor, he or she will likely have prescribed some pain relieving medication after you've been diagnosed with a shoulder fracture.
The reason for this is that typically shoulder fractures are often painful the first few weeks so it is important to take your painkillers regularly to manage the pain and still participate in daily activities and moving around.
3) Exercises
In the beginning or early stages, you need to be very patient and cautious - you need to rest your shoulder and not move it at all until your doctor have given you the go-ahead to start moving your shoulder.
The reason for this is to protect your shoulder and ensure that the fractured parts stabilize and heal well together. If you keep moving your fractured shoulder when you're not supposed to, that may lead to a complication of non-union or mal-union.
Of course you will be encouraged to move all your non-injured joints and body parts, such as your elbow, wrist, fingers, neck and body etc. You can go for walks and move around in a sling, or even go to work if it's safe for you to do so and if your work is moreso sedentary or desk bound.
Once you review with your shoulder shoulder and as soon as your doctor is medically and professionally satisfied that your shoulder fracture is healing well (typically you will need to review and meet up with them regularly as well as do regular x-rays to see how your fracture is healing), then your shoulder doctor will refer you to our senior physiotherapists for shoulder fracture physiotherapy.
We will then start you on a range of mobility exercises to improve and ultimately restore the range of movement in your affected shoulder. Most of the time that begins in about 2 - 4 weeks after the injury happened.
We will typically start with shoulder pendular exercises (passive ranging) and then active assisted exercises (active assisted mobilization) where you use your good arm to support and move the broken arm.
In some cases, you may be placed onto a pulley system to help stretch out your affected shoulder.
Our senior physiotherapists will start you immediately on hand, forearm, wrist and finger strengthening exercises immediately, and within a few weeks after we may start gentle and protected shoulder strengthening exercises.
To be safe, we will start with isometric strengthening (where the muscles contract without shortening or lengthening) where there is no shoulder movement.
Within 6 - 10 weeks, if your shoulder fracture is healing well, we will progress you onto advanced shoulder strengthening exercises.
4) Surgery
Fortunately, only around 10-20% of shoulder fractures injuries end up requiring corrective surgery. Shoulder surgery is required if:
- The bone fragments are displaced (moved from original position)
- The bone has punctured the skin, known as an open fracture
- Bone fragment has damaged the surrounding nerves or blood vessels
- There is damage to the parts of the bone where the rotator cuff muscles attach
- If the damage affects the surfaces of the shoulder joint
- If there is a fracture dislocation – where the shoulder joint has dislocated as well as been broken
- If more than one of the shoulder bones is fractured
- If the fracture fails to heal, known as non-union (basically the fractured parts healing separately of each other)
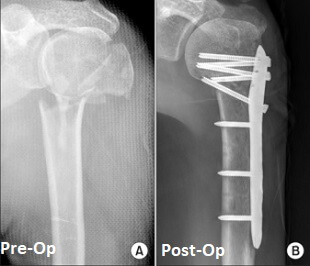
Surgery for a shoulder fracture mainly focuses on
- realigning the bones
and then
- stabilizing/fixing them in place with either plates, screws or rods
Unfortunately if there is significant damage to the humeral head which cannot be fixed, salvaged or repaired (the surgeon will try their best to), then they have no choice but to get the top part of the humerus replaced, and this procedure is known as a hemiarthroplasty or partial shoulder replacement.
Following corrective shoulder surgery, treatment is very similar to the non-surgical treatment with a period of immobilization in a sling and then progressing through a shoulder physiotherapy program under the guidance of our senior physiotherapists.
Recovery after Shoulder Fracture
Following a shoulder fracture, be it managed conservatively without shoulder surgery or with corrective surgery, patients should expect recovery time between 8 to 12 months (up to 1 year).
Full recovery from a shoulder fracture, where it is treated surgically or not, can take 6-12 months. It is very important to get the right balance between allowing the fracture time to heal while also trying to prevent stiffness.
Also, there is a constant battle and struggle between:
- letting / giving the shoulder fracture more time to heal versus
- mobilizing the shoulder to prevent shoulder stiffness (and possibly prevent onset of conditions similar to frozen shoulder)
Typically, younger patients (below 45 years of age) will be able to achieve 100% of shoulder strength and movement, as compared to older patients above 45 years of age tends to not always achieve full shoulder strength and movement. Of course, our senior physiotherapists will always strive for 100% recovery back to normal.
Yes we get it too, that many patients and individuals are often afraid of moving their shoulder after a shoulder fracture for fear of:
- pain
- re-injury or refracture
...but most of the time, we can safely say it's more so due to 'uncertainty' - they may not be sure how much can they move, do they move the shoulder despite pain ie "do they push past pain" etc - I'd like to confidently assure you that we only bring in very experienced senior physiotherapists with years if not decades of clinical experience to help guide you to full shoulder movement recovery.
Some of shoulder physiotherapy modalities that we will provide includes:
- cold therapy
- moist heat paraffin wax therapy
- radio-frequency Indiba physiotherapy to accelerate soft tissue healing
- joint mobilization
- stretching exercises
- strengthening exercises
- scar management
- hands on manipulation and mobilization (manual therapy)
- computerized spinal decompression traction
- soft tissue management
- heat therapy and heat treatment and heat pack to relief tight muscles and joints
- ultrasound therapy to accelerate soft tissue healing
- exercise therapy
- acupuncture and/or dry needling
- deep tissue release
- and more
Don't worry, we will advise you step by step on how much you can move your shoulder, when you can push it and how much you can grow - we're with you all the way.
getting back to daily life after a shoulder fracture
1) Showering And Washing Up
It's usually very ok and safe to remove your sling to shower after a shoulder fracture. Unless you have a recent shoulder fracture and a wound, then get your wound covered with a water-proof dressing first or replace the wound dressing after.
Do try to be seated to shower as your balance may be impaired
due to the shoulder injury. It's always very refreshing to be able to
shower and clean up - the best way to wash your arm pit is to lean
forward such that your affected arm is away from your body (similar to
pendulum exercises) and then you wash using your unaffected hand.
2) Wound Care
If
you have had corrective shoulder surgery please understand that you
have to keep the wound clean and dry for the first 7-10 days. If you wet
the dressing, please connect with us for an orthopedic wound care session.
3) Changing Clothing And Getting Dressed
Again, most of the time it'd be fairly ok but it's just something you need to wrap your mind around and practice a little - you'll get the hang of it very quickly.
Firstly you need to think about stuff you're gonna wear.
- Always change or dress in sitting - it's much easier and not to mention, safer.
- Button down tops are easiest, and easy too when they're loose. For tops, wear on the affected arm first.
- For pants, choose looser ones and with rubber bands is easier, without having the need for buckling or belt or tying.
- For bras, it's much easier to clip at the front and slowly move it to the back
Generally tight clothing is tougher as it "sticks" to your body so it can be challenging to wear or remove.
4) Smoking
There is research that demonstrates clearly that smoking delays healing and health, and definitely impacts fracture healing so you may want to consider stopping smoking entirely or at least stop smoking until your shoulder fracture has healed.
5) Exercises
At the core of what we do is medically safe and proven exercises to protect and improve movement and health. Our senior physiotherapists will assess your shoulder and teach and guide your shoulder physiotherapy rehabilitation and exercises.
Our senior physiotherapists will also teach you shoulder exercises which you should do at least 2-4x per day to
- decrease shoulder stiffness
- improve shoulder movement
- improve shoulder strength
- accelerate shoulder use and recovery
Yes we know sometimes it is painful and not fun (we'll try our best to make it engaging and fun ok =D) and preservere with us as we help you to achieve 100% shoulder strength and movement.
6) Can I Drive?
Usually the doctors and us will not recommend driving for a while, and the reason being:
- your shoulder need some time with shoulder physiotherapy and healing to improve its shoulder and strength for steering to drive safely (typically 8-12 weeks)
- any motor vehicle accidents may cause reinjury which slows down shoulder fracture
Be patient and we will help you to get back to normal living, driving, working as per normal as soon as we can ok =)
7) Work
You may be able to go back to work earlier if your work can be done with 1 hand or is deskbound or consultative in nature.
Typically patients cannot go back to work for at least 6 weeks to 12 weeks, but in some cases, if the work is less physically demanding and moreso consultative or deskbound, it may be a good idea to return to work on a part time or full time basis.
Of course it also matters if it's your dominant hand that has the shoulder fracture compared to non-dominant hand.
8) Sports
We prefer to be very safe and conservative, so we recommend no contact sports for at least 6 months until your shoulder fracture has 100% healed.

Reference Sources