|
BOOK NOW |
ASK ABOUT YOUR PAIN |
Home > Blog > Physiotherapy > Shoulder Impingement Physiotherapy
Shoulder Impingement Physiotherapy
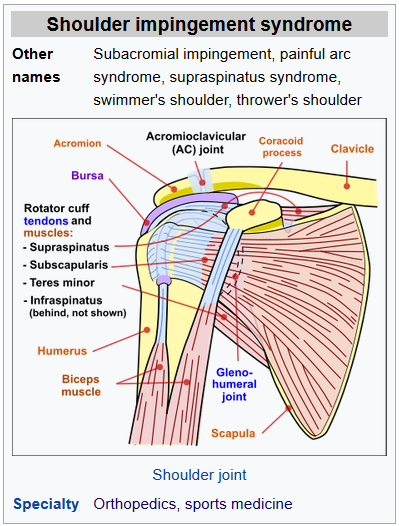
Shoulder impingement syndrome is a syndrome involving tendonitis (inflammation of tendons) of the rotator cuff muscles as they pass through the subacromial space, the passage beneath the acromion.
It is particularly associated with tendonitis of the supraspinatus muscle. This can result in pain, weakness and loss of movement at the shoulder.
Signs and symptoms
The most common symptoms in impingement syndrome are
- pain
- weakness
- loss of movement at the affected shoulder
The pain is often worsened by shoulder overhead movement and may occur at night, especially when lying on the affected shoulder. The onset of the pain may be acute if due to an injury or insidious if due to a gradual process such as an osteoarthritic spur.
The pain has been described as dull rather than sharp, and lingers for long periods of a time, making it hard to fall asleep. Other symptoms can include a grinding or popping sensation during movement of the shoulder.
The range of motion at the shoulder may be limited by pain. A painful arc of movement may be present during forward elevation of the arm from 60° to 120°. Passive movement at the shoulder will appear painful when a downwards force is applied at the acromion but the pain will ease once the downwards force is removed.
How Does it Feel?
Individuals with shoulder impingement may experience:
- Restriction in shoulder motion with associated weakness in movement patterns, such as reaching overhead, behind the body, or out to the side.
- Pain in the shoulder when moving the arm overhead, out to the side, and beside the body.
- Pain and discomfort when attempting to sleep on the involved side.
- Pain with throwing motions and other dynamic movement patterns
Causes of shoulder impingement
When the patient's arm is raised, the subacromial space (gap between the anterior edge of the acromion and the head of the humerus) narrows; the supraspinatus muscle tendon passes through this space.
Anything that causes further narrowing has the tendency to impinge the tendon and cause an inflammatory response, resulting in shoulder impingement syndrome. Such causes can be
- bony structures such as subacromial spurs (bony projections from the acromion),
- osteoarthritic spurs on the acromioclavicular joint, and
- variations in the shape of the acromion
Thickening or calcification of the coracoacromial ligament can also cause impingement.
Loss of function of the rotator cuff muscles, due to injury or loss of strength, may cause the humerus to move superiorly, resulting in impingement. Inflammation and subsequent thickening of the subacromial bursa may also cause impingement.
Weight training exercises where the arms are elevated above shoulder height but in an internally rotated position such as the upright row have been suggested as a cause of subacromial impingement. Another common cause of Impingement syndrome is restrictions in the range movement of the scapulo-thoracic surfaces.
Commonly, a rib (or ribs) between rib 2 and rib 7/8 on the side of the impingement, may jut out slightly and/or feel hard when the person springs on it/them. When this occurs, the scapula is raised and anteverted (angled forwards).
This in turn pushes the acromion and the humeral head out of its usual anatomical position placing pressure downwards at the head of the humerus at the position of the nerve thus causing the impingement syndrome.
This is visibly demonstrated by a slightly raised and protracted shoulder girdle. Note: the humerus anteverts in this position causing a more protrusive section of the humerus to press upwards towards the acromion.
Mechanism
The scapula plays an important role in shoulder impingement syndrome.
It is a wide, flat bone lying on the posterior thoracic wall that provides an attachment for three different groups of muscles. The intrinsic muscles of the scapula include the muscles of the rotator cuff- the subscapularis, infraspinatus, teres minor and supraspinatus.
These muscles attach to the surface of the scapula and are responsible for the internal and external rotation of the glenohumeral joint, along with humeral abduction. The extrinsic muscles include the biceps, triceps, and deltoid muscles and attach to the coracoid process and supraglenoid tubercle of the scapula, infraglenoid tubercle of the scapula, and spine of the scapula. These muscles are responsible for several actions of the glenohumeral joint.
The third group, which is mainly responsible for stabilization and rotation of the scapula, consists of the trapezius, serratus anterior, levator scapulae, and rhomboid muscles and attach to the medial, superior, and inferior borders of the scapula. Each of these muscles has their own role in shoulder function and must be in balance with each other in order to avoid shoulder pathology.
Abnormal scapular function is called scapular dyskinesis. One action the scapula performs during a throwing or serving motion is elevation of the acromion process in order to avoid impingement of the rotator cuff tendons. If the scapula fails to properly elevate the acromion, impingement may occur during the cocking and acceleration phase of an overhead activity.
The two muscles most commonly inhibited during this first part of an overhead motion are the serratus anterior and the lower trapezius. These two muscles act as a force couple within the glenohumeral joint to properly elevate the acromion process, and if a muscle imbalance exists, shoulder impingement may develop.
The scapula may also be misplaced if a rib deep to it is not moving correctly. Often in the case of Shoulder Impingement Syndrome, the scapula may be anteverted such that the shoulder on the affected side appears protracted. The ribs that may cause such an anteversion of the scapula include ribs 2-8.
Diagnosing shoulder impingement
Impingement syndrome can be diagnosed by a targeted medical history and physical examination, but it has also been argued that at least medical imaging (generally X-ray initially) and/or response to local anesthetic injection is necessary for workup.
On physical exam, the physician may twist or elevate the patient's arm to test for reproducible pain (the Neer sign and Hawkins-Kennedy test). These tests help localize the pathology to the rotator cuff; however, they are not specific for impingement. Neer sign may also be seen with subacromial bursitis.
Response to local anesthetic
The physician may inject lidocaine (usually combined with a steroid) into the bursa, and if there is an improved range of motion and decrease in pain, this is considered a positive "Impingement Test".
This approach not only supports the diagnosis for impingement syndrome, but is also therapeutic.
Imaging
Plain x-rays of the shoulder can be used to detect some joint pathology and variations in the bones, including acromioclavicular arthritis, variations in the acromion, and calcification. However, x-rays do not allow visualization of soft tissue and thus hold a low diagnostic value.
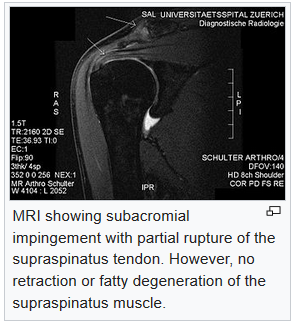
Ultrasonography, arthrography and MRI can be used to detect rotator cuff muscle pathology. MRI is the best imaging test prior to arthroscopic surgery.
Due to lack of understanding of the pathoaetiology, and lack of diagnostic accuracy in the assessment process by many physicians, several opinions are recommended before intervention.
Treatment
Impingement syndrome is usually treated conservatively, but sometimes it is treated with arthroscopic surgery or open surgery. Conservative treatment includes
- rest
- decreasing, modifying or stopping painful activities
- shoulder physiotherapy
Physical therapy treatments would typically focus at maintaining range of movement, improving posture, strengthening shoulder muscles, and reduction of pain. NSAIDs and ice packs may be used for pain relief.
Steroids
Therapeutic injections of corticosteroid and local anaesthetic may be used for persistent impingement syndrome. The total number of injections is generally limited to three due to possible side effects from the corticosteroid.
Side note: A 2017 review found corticoestroid injections only give small and transient pain relief.
Surgery
A number of surgical interventions are available, depending on the nature and location of the pathology. Surgery may be done arthroscopically or as open surgery. The impinging structures may be removed in surgery, and the subacromial space may be widened by
- resection of the distal clavicle
- excision of osteophytes on the under-surface of the acromioclavicular joint.
Damaged rotator cuff muscles can be surgically repaired. A 2019 review found that the evidence does not support decompression surgery in those with more than 3 months of shoulder pain without a history of trauma.
shoulder impingement physiotherapy

It is important to get proper treatment for shoulder impingement as soon as it occurs. Secondary conditions can result from the impingement of the tissues in the shoulder, including irritation of the bursa and rotator-cuff injuries, tendinitis or tears.
Patients can be assured that physical therapy (also known as physiotherapy) can be very successful in treating shoulder impingement syndrome. Our senior physiotherapists will provide and indepth assessment and then devise a customized physio treatment plan that is specific to your condition and goals.
Your individual treatment program may include:
Pain Management. Our senior physiotherapists will help you identify and avoid painful movements, as well as correct abnormal postures to reduce impingement compression. Therapeutic modalities, like iontophoresis (medication delivered through an electrically charged patch) and ultrasound therapy to accelerate soft tissue healing. Cold therapy may also be helpful to reduce pain.
Manual Therapy. Our senior physiotherapists will use manual therapy techniques, such as gentle joint movements, soft-tissue massage, and shoulder stretches to get your shoulder joint gliding and moving properly, so that the tendons and bursa in the shoulder decrease and avoid impingement.
Range-of-Motion Exercises. You will learn exercises and stretches to help your shoulder and shoulder blade move properly, so you can return to reaching and lifting without pain.
Strengthening Exercises. Our senior physiotherapists will determine which strengthening exercises are right for you and your impinged shoulder, depending on your specific condition and severity.
Often with shoulder impingement syndrome, the head of the humerus tends to drift forward and upward due to the rotator-cuff muscles becoming weak. Strengthening the rotator-cuff and scapular muscles helps position the head of the humerus bone down and back to ease the impingement.
You may also perform
resistance training exercises to strengthen your weaker muscles.